Physical Therapy for Longevity — Clovis, California
Stretching or home exercises didn’t solve your pain.
So what will?
David Quenzer, DPT
David and his bride


17,000+ hours of hands-on experience solving complex pain
This first visit isn’t a typical consultation. You are treated, and if there’s a change we both feel, I offer the opportunity to continue working with me in an all-in solution for you. Getting up off the floor, turning your head to check your blind spot, going downstairs, or even running. We test it all before and after this visit, so you can see for yourself whether there’s a real benefit for you.
Problems I solve:
Low Back Pain
Sciatica
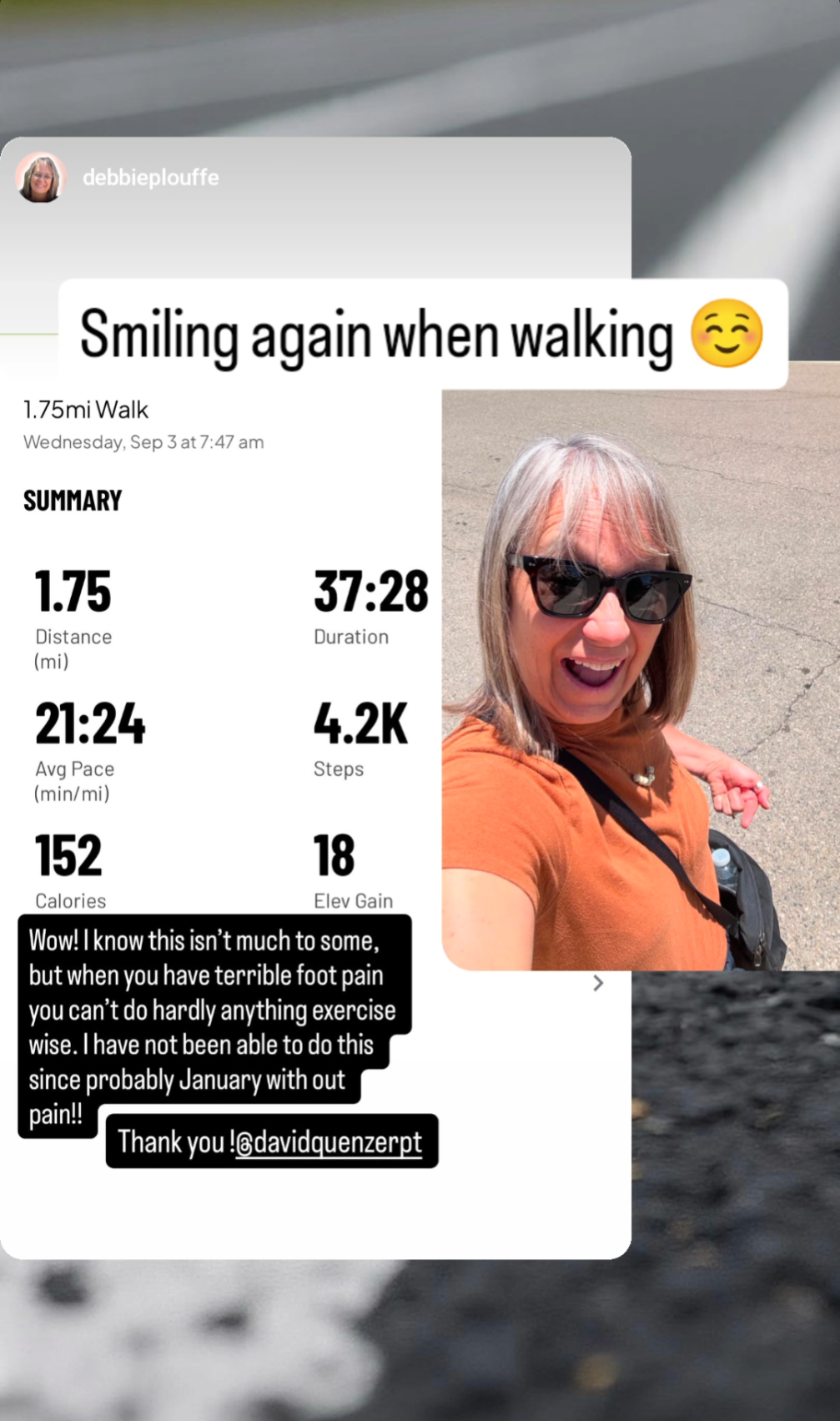
Plantar Fasciitis
Shoulder Pain
Neck Pain & Headaches
Hip Pain
Knee Pain
Balance & Falls
Men’s Pelvic Health
Women’s Pelvic Health
Start Your Recovery
↑ Your first visit is free — the only way to know if this will work for you
Prefer to talk first? Call me (559) 549-6282